77. Can you have anaphylaxis with high blood pressure?
Yes.
The misconception that a person with high blood pressure cannot be experiencing anaphylaxis is enduring and dangerous.
Author’s note: Thanks to the intrepid reader who caught a big typo right here. When I published the post, it said, “The misconception that a person with high blood pressure can be experiencing anaphylaxis is enduring and dangerous.” This is a whopper mistake. It should say, “The misconception that a person with high blood pressure canNOT be experiencing anaphylaxis is enduring and dangerous.” You CAN have high blood pressure and anaphylaxis at the same time. Thanks again!
Lots of providers (and patients) think that high blood pressure rules out anaphylaxis. This is not true.
This misunderstanding comes from confusing two closely related but distinct concepts: anaphylaxis and anaphylactic shock.
Anaphylaxis is a severe allergic reaction affecting multiple organ systems.
Anaphylactic shock is when anaphylaxis causes such poor blood circulation that the heart cannot pump out enough blood to the body.
Anaphylactic shock is a form of circulatory shock, which means exactly what I just described: oxygenated blood is not being pumped out of the heart and through the blood vessels to the tissues that need it.
Anaphylactic shock is defined as blood pressure 30% below the patient’s baseline or a systolic blood pressure below 90 mm Hg. The systolic blood pressure is the top number when you get your blood pressure checked. If that top number is below 90 mm Hg, and that is the result of anaphylaxis, you are in anaphylactic shock.
Anaphylactic shock is the most serious potential complication of anaphylaxis. Anaphylactic shock happens when the chemicals released by mast cells cause a lot of the fluid in the bloodstream to “fall out” of the bloodstream and get stuck in the tissues.
When this happens, that fluid loss causes the blood pressure to drop. In response, the heart beats faster to try and use the blood it still has left to get oxygen to the body. However, at a certain point, even beating really fast is not enough to get enough blood to the tissues. At this point, shock sets in.
Anaphylactic shock occurs specifically as a result of low blood pressure. Because of this, providers strongly associate low blood pressure with anaphylaxis. They may not realize that while a person with high blood pressure cannot be having anaphylactic shock, they can be having anaphylaxis.
Part of the confusion is that anaphylaxis has been defined lots of different ways by many different groups. I have written a very detailed post about this (see the link below). Even today, exactly what constitutes anaphylaxis not agreed upon by everybody.
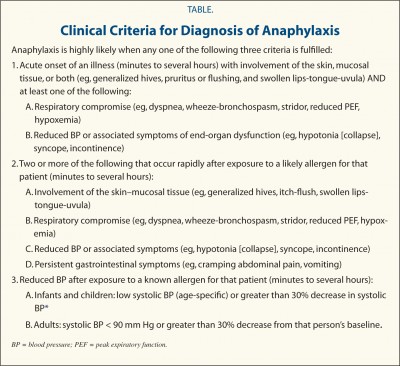
The most widely used criteria in the US are the criteria published in 2006 by the World Allergy Organization journal. These criteria explicitly state that a person does not need to have low blood pressure to be having anaphylaxis. A person can meet these criteria based upon a variety of combinations of symptom and vital signs that do not include low blood pressure.
2006 WAO Anaphylaxis Criteria
For additional information, please visit the following posts:
60. Is anaphylaxis the same as anaphylactic shock?
No. Anaphylaxis can result in anaphylactic shock but it often doesn’t. When talking about anaphylactic shock, people are referring to circulatory shock that was caused by anaphylaxis. Circulatory shock occurs when there is not enough blood to carry oxygen to all the tissues that need it. When the tissues don’t get enough oxygen, your organs stop working correctly.
Circulatory shock is usually caused by low blood pressure. Anaphylaxis commonly causes low blood pressure and that can cause shock. However, anaphylaxis does not always cause low blood pressure, and it does not always cause shock.
61. If a tryptase level over 10.9 ng/mL is high, why is one of the criteria for systemic mastocytosis a tryptase level of 20.0 ng/mL or higher?
Tryptase level is used in two ways in assessing mast cell patients: as a marker for activation, and as a marker for how many mast cells are in the body.
There are two primary methods of using tryptase to indicate mast cell activation.
The first way is to compare a tryptase level when a patient is reacting to a tryptase level when they are not reacting (baseline). Mast cells release more tryptase when they are activated. For mast cell patients, an increase of 20% + 2 ng/mL is considered evidence of mast cell activation. So if a patient has a baseline tryptase of 5 ng/mL when they are not reacting, anything 8 ng/mL (20% of 5 ng/mL is 1 ng/mL, then add 2 ng/mL = 8 ng/mL) or higher is considered evidence of activation.
The second way is to count anything over 10.9 ng/mL as evidence of activation.
When you are using tryptase as a measure of how many mast cells are in the body, the patient should not be reacting beyond their normal day to day symptoms. This is because you don’t want an increase in tryptase from activation to make the baseline level look higher than it is. Tryptase is used to measure how many mast cells are present because mast cells release some tryptase all the time, even when they aren’t activated.
Anything over 10.9 ng/mL is considered an elevation of tryptase. The reason that 20 ng/mL is the cutoff for the SM criterion is that patients are likely to have a positive bone marrow biopsy when the tryptase level is twice normal (21.8 ng/mL). They round the number down to 20 ng/mL because all tests have a margin of error. By rounding down to 20 ng/mL, they catch patients that might not have made the cutoff before because of an error in the test. This means that a patient who has a tryptase level of 20 ng/mL or higher is likely to have a bone marrow biopsy that will be positive for systemic mastocytosis.
For more detailed reading, please visit these posts:
Author’s note: I am not a medical doctor. Anaphylaxis and use of epinephrine must be discussed with the managing provider to determine the best treatment plan for any individual patient.
Determination of mast cell reaction vs anaphylaxis
Anaphylaxis has a very complicated relationship with mast cell disease. Mast cell symptoms and reactions are inherent parts of mast cell disease. All mast cell patients can reasonably expect to have some mast cell symptoms as part of their baseline.
Anaphylaxis is not an inherent part of mast cell disease. Anaphylaxis is a complication of mast cell disease. Mast cell patients are at increased risk for anaphylaxis, but not all mast cell patients experience anaphylaxis. In some studies, as many as 50% of mast cell patients had never experienced anaphylaxis.
The fact that anaphylaxis and mast cell reactions can have the same symptoms is probably the reason why it is difficult to separate the two. So for a minute, let’s stop talking about mast cell disease and consider a similar scenario that is better described.
Coronary artery disease (CAD) is the leading cause of death worldwide. It affects millions of people around the world. Everyone knows someone with coronary artery disease. Probably multiple someones.
Patients with CAD have narrow arteries that interfere with blood flow to the heart. When they are diagnosed with CAD, their provider will tell them about symptoms they may experience daily as a normal part of their disease. Their provider will also tell them about symptoms that they may experience that indicate the heart is not getting enough oxygen, like radiating chest pain, shortness of breath and nausea. In these scenarios, the patient needs to take a med like nitroglycerin to try and stop the episode. If that doesn’t work, the patient is at risk for a heart attack.
Radiating chest pain, shortness of breath and nausea are symptoms of CAD. Heart attack is not a symptom of CAD. It is a complication of CAD. It can also present with the same symptoms of radiating chest pain, shortness of breath and nausea.
Flushing, nausea, diarrhea and hives are symptoms of mast cell disease. (I’m just using these as examples, there are many others). Anaphylaxis is not a symptom of mast cell disease. It is a complication of mast cell disease. It can also present with the same symptoms of flushing, nausea, diarrhea and hives.
These are the potential scenarios when a mast cell patient starts experiencing more severe symptoms than usual.
The patient experiences flushing, nausea, diarrhea and hives. They don’t take rescue meds and the symptoms resolve. This is a mast cell reaction. This is not anaphylaxis.
The patient experiences flushing, nausea, diarrhea and hives. They take rescue meds (not including epi here) and the symptoms resolve. This is a mast cell reaction. This is not anaphylaxis.
The patient experiences flushing, nausea, diarrhea and hives. They may or may not take rescue meds (not including epi here). Either way, the symptoms do not resolve. The amount of mast cell degranulation triggers a large scale reaction that initiates anaphylaxis. This is anaphylaxis and requires epinephrine. There are two possibilities here: it was anaphylaxis from the beginning, or it started as a mast cell reaction and became anaphylaxis. Either way, it requires epinephrine and other rescue meds.
It seems to me that when anaphylaxis occurs in mast cell patients as a sudden onset event that the symptoms seen are usually distinct from regular mast cell reaction symptoms. (This last sentence is based upon what I have experienced and what is reported to me by patients. There is no data on this.)
General notes on use of epinephrine
How do you know it is anaphylaxis? That’s the hard part. Mast cell experts feel differently about this. Most say to only use epi if you have trouble breathing or low blood pressure because then you know it is life threatening and thus anaphylaxis and not a mast cell reaction.
If you are having trouble breathing or low blood pressure (for adults, under 90 systolic), that is generally cited as the appropriate point to use epi. However, it is a conversation and decision that must be made with you and a doctor that knows you and your disease.
If you have had an episode before where you had severe symptoms and recovered without epinephrine, it is phenomenally unlikely that it was anaphylaxis.
If you think you may need epinephrine and are unsure, it is generally recommended to use your epipen. The reason for this is that epinephrine is pretty safe, despite how the movies depict it. The risk of using an epipen when you don’t need it is side effects of epinephrine use: rapid heartbeat, elevated blood pressure, anxiety, and generally not feeling great for a day or so. The risk of not using an epipen when you need it is death. People die from anaphylaxis with their epipens on them unused.
Meeting diagnostic criteria for anaphylaxis
As I reviewed in the previous post, there are many sets of diagnostic criteria for anaphylaxis. The one that is the most widely used in the WAO criteria published in 2006. This set of criteria has been validated, meaning it was effective for correctly identifying patients experiencing anaphylaxis while excluding those who weren’t. Even still, they note that about 5% of patients with anaphylaxis will not be covered by these criteria and to use discretion with this population.
The 2006 WAO criteria (shown below) are often used by emergency departments to determine whether or not epinephrine is needed. If the patient meets the criteria, epi is warranted. This is one of the reasons why anaphylaxis is often considered synonymous with requirement of epinephrine.
2006 WAO Anaphylaxis Criteria
Determining whether or not you have anaphylaxis when your blood pressure is not very low and you can breathe fine is not straightforward for mast cell patients. There are several charts that are often posted in mast cell groups that show four or five stages of anaphylaxis. These charts are designed for people who do not have baseline allergic symptoms. Mast cell patients have baseline allergic symptoms.
If you have mast cell disease and have flushing, nausea and hives regularly, that is not grade II anaphylaxis. That is mast cell disease. Symptoms that are part of your normal baseline or reaction profile do not contribute to the overall assessment of anaphylaxis. So let’s assume I have flushing, nausea and hives every day. But then one day I also have diarrhea and tachycardia, which isn’t normal for me. That is grade III anaphylaxis per the Ring and Messmer scale (shown below). Whether or not you use epi at that point, assuming your blood pressure is not low and you can breathe okay, depends upon whether or not your doctor endorses the use of that scale.
Ring and Messmer Anaphylaxis Grading Scale
Anaphylaxis vs anaphylactic shock
I often see people use anaphylaxis and anaphylactic shock interchangeably. They’re not the same thing.
Anaphylaxis is a severe, multisystem allergic reaction.
Shock is more properly called circulatory shock. It is a state arising from poor circulation such that tissues are not receiving sufficient blood supply. Weak pulse, tachycardia, low heart rate, and mental status changes including loss of consciousness are all symptoms of shock.
Anaphylactic shock is circulatory shock caused by low blood pressure due to the vasodilation from large scale degranulation. By definition, it is blood pressure 30% below the patient’s baseline or below standard values (90 systolic for adults). So if you aren’t experiencing circulatory shock, you aren’t having anaphylactic shock.
References:
Sampson HA, et al. Second symposium on the definition and management of anaphylaxis: summary report – Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol 2006: 117(2), 391-397.
Brown, SGA. Clinical features and severity grading of anaphylaxis. Journal of Allergy and Clinical Immunology 2004: 114(2), 371-376.
Sampson HA, et al. Symposium on the definition and management of anaphylaxis: summary report. J Allergy Clin Immunol 2005; 115(3), 584-591.
Ring J, et al. History and classification of Anaphylaxis. Chem Immunol Allergy 2010: 95, 1-11.